
Your Hip
- About Your Hip
- What Can Go Wrong
- Non-Invasive Treatments
- Hip Injections
- Direct Anterior Hip Replacement
- Mini-Posterior Hip Replacement
- Revision Total Hip Replacement for failed hip implants
- SHARED DECISION MAKING: TOTAL HIP REPLACEMENT (Required completion by all patients undergoing surgery by Dr. Martin)
About Your Hip
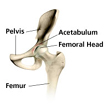
The hip joint is what is known as a “ball and socket” joint. It is a large joint made up of a ball (which is attached to the upper part of the thigh bone called the femur) and a socket (called the acetabulum, this structure is part of the pelvis). The hip joint is only second to the shoulder for allowing the most motion of any joints in our body. The hip joint is a true weightbearing joint and often sees a load of about 4 times the weight of our bodies with normal daily activity. The joint is lined with a spongy material called cartilage, which cushions the joint. The hip is surrounded by strong muscles which work to move and support the joint.
Figure 1. Shows a healthy appearing hip joint.
Because the hip joint is so important allowing us to walk, run, and jump, when we develop a problem with the joint it can interfere with our quality of life and our ability to function and do the things we like or need to do.
.
What Can Go Wrong
When hip problems occur they are often felt as pain in the groin area, the front of the thigh or sometimes in the knee. Pain can be felt on the side of the hip as well. (Pain felt in the buttock or back of the leg is usually not a hip problem.) Hip problems also can cause stiffness, limping, and difficulty bending over to tie the shoes or even get dressed. The following are the most common reasons we see people presenting with hip problems:
- Osteoarthritis: this is a mechanical condition where the cushion on the ends of the joints wears out. For more information watch this video: https://www.youtube.com/watch?v=bUvlbbz3K2c
- Hip Fractures: these usually occur as a result of osteoporosis (weaking of the bones with aging) and a fall or a high energy trauma. Inability to bear weight on the leg and significant pain are symptoms. If this is suspected, immediately go to an emergency room for evaluation. It is important to know that hip fractures do not always show up on x-rays, and sometimes an MRI or other imaging is necessary to diagnose a fracture
- Inflammatory arthritis: this includes rheumatoid arthritis, psoriatic arthritis and others. The commonality here is that something systemic is going on where the hip joint is being attacked. Often times medical treatments are effective in the early stages of disease
- Bursitis and tendonitis: this is an inflammation around the joint either in the muscles or the bursa.
- Osteonecrosis (avascular necrosis): this is a condition where blood supply to the ball of the hip gets disrupted. This can occur with steroid use, alcohol use, trauma, or in many cases the cause is unknown. Over time the head can collapse and the joint can become arthritic.
- Other issues: certainly there can be other serious issues which can occur around the hip such as tumors, nerve damage, etc. Symptoms should never be ignored and care should be obtained by a physician.
For more information on the hip and thigh visit the American Academy of Orthopaedic Surgeons visit: http://orthoinfo.aaos.org/menus/hip.cfm
.
Non-Invasive Treatments
Surgery should be considered a last resort. There are some basic things which should always be tried prior to considering surgical intervention. These include:
- Weight Loss (if needed): The hip joint sees the force of 4 times the weight of the body with most normal daily activity. So if you are carrying around 50 extra pounds, that is felt as 200 pounds of ADDITIONAL pressure on the joint. Lose the weight, and the joint will feel better. Even if it doesn’t, you will be in better health, feel better about yourself and be a safer candidate for surgery. *always consult a physician prior to changing diet/attempting weight loss
- Exercise: Numerous studies have demonstrated the beneficial effects of exercise for your hips. Strong muscles can support the joint and take pressure off. They can also help you walk and function better. Movement in the joint is important to keep it from getting stiff. Click here to print a hip conditioning program: http://orthoinfo.aaos.org/PDFs/Rehab_Hip_3.pdf *always consult a physician prior to starting any new exercise program
- Medications: Numerous medications, including acetaminophen (common brand: Tylenol), anti-inflammatories (common brands over the counter: advil, motrin, alleve, common brands presecription: Celebrex, Voltaren, Mobic), and tramadol (common brand: Ultram) all can be effective in controlling pain and symptoms associated with hip problems. Medications, even over the counter, can be associated with significant risks though and you should always consult with a physician prior to utilizing.
- Supplements: Several supplements, although controversial, possibly may alleviate the symptoms of hip arthritis and pain, with less of a risk than traditional medications. These include glucosamine sulfate (http://www.nlm.nih.gov/medlineplus/druginfo/natural/807.html) and Tumeric/Curcumin (http://www.nlm.nih.gov/medlineplus/druginfo/natural/662.html)
- Topical treatments: Numerous topical treatments may temporarily help including menthol based products, capsaicin, and others.
Hip Injections
Currently, hip injections are a way to alleviate symptoms and possibly delay the need for surgery. Injections to do not cure arthritis. Since the hip is deep, injections are generally done under image guidance (either with a fluoroscope/x-ray machine or with ultrasound. Numerous substances can be injected including:
- Cortisone: this is a powerful anti-inflammatory injected right into the joint. It tends to work quickly with patients experiencing relief usually within a week. The time in which the effects last are variable, but a good result is considered to be 3 months or more.
- Hyaluronic Acid: This substance, FDA approved for and commonly used in the knee, is not FDA approved for use in the hip. Its use is considered off-label and is not typically covered by insurance. It is used widely and approved in Europe, Canada, and Australia. Numerous studies support possible effectiveness in helping with hip symptoms. It does not cure arthritis or regrow cartilage
- Platelet Rich Plasma (PRP) and Stem cells: These so called “biologic” treatments are relatively new and untested. There is little science to support their use at this time and they are not covered by insurance. There is no convincing evidence that they alter the course of arthritis or regrow cartilage.
Direct Anterior Hip Replacement
If non-operative treatments have failed and the hip needs to be replaced, there is good news. A new and innovative way of replacing the hip joint without cutting any muscle was developed and has been perfected. Direct Anterior Hip Replacement using the innovative HANA table allows patients to get back on their feet almost immediately without the usual restrictions and precautions and potentially less pain! The technique utilizes a 3 to 4 inch incision on the front (anterior) of the thigh. An interval is utilized between the muscles in order to limit soft tissue trauma. Not cutting these muscles potentially reduces the risk of dislocation and may allow for an accelerated recovery.
Figure 2. This is a picture of the HANA table.
 This high tech table allows the patient to be lying on their back during the surgery allowing a level of precision to be achieved which is generally not possible with surgery where the patient is lying on their side.
This high tech table allows the patient to be lying on their back during the surgery allowing a level of precision to be achieved which is generally not possible with surgery where the patient is lying on their side.
The procedure allows the use of intraoperative x-ray to ensure the components are put in properly and that leg lengths are being matched to the opposite side.
Video 1. Shows how the positioning and leg lengths are accurately reproduced.
Dr. Martin has performed direct anterior approach hip surgery for the past 5 years and has become a big proponent of the technique because of the ease of recovery for patients, but perhaps more importantly, the precision of implant placement which is required for a good long term outcome.
To watch an animation of the anterior surgical technique, see below:
To better understand what is done with hip replacement, see below:
To watch a live surgery of the technique (caution: this involves graphic content which may not be suitable for all viewers), performed at the Brigham and Women’s Hospital where Dr. Martin completed his fellowship in hip and knee replacement, click this link: Direct Anterior Approach for Total Hip Arthroplasty
To Download a Brochure on Direct Anterior Hip Surgery, see below:
English: http://patients.depuyorthopaedics.com/binary/org/DEPUY/doc/pt.com/0612-55-
502r8_AA.pdf
Spanish: http://patients.depuyorthopaedics.com/binary/org/DEPUY/doc/pt.com/0612-61-
508r1.pdf
.
Mini-Posterior Hip Replacement
Although Direct Anterior Hip Replacement using the HANA table, has become Dr. Martin’s preferred method of hip replacement, it is not possible in all patients. Some patients with prior surgery and hardware, birth defects and other issues require a posterior approach. Posterior approach surgery remains the most common way hip replacement is performed in this country. For over 10 years, Dr. Martin has performed a less invasive variant of posterior hip replacement, called Mini-Posterior Hip Replacement.
To better understand what is done with total hip replacement, see below:
To Download a Brochure on Total Hip Replacement Surgery, see below:
English: http://patients.depuyorthopaedics.com/binary/org/DEPUY/doc/pt.com/0609-45-
000r10.pdf
Spanish: http://patients.depuyorthopaedics.com/binary/org/DEPUY/doc/pt.com/0610-76-
000r4_SP_THR.pdf
.
Revision Total Hip Replacement
Dr. Martin has special expertise in performing surgery in hips that have already been operated on. This is called Revision Total Hip Replacement and is required generally due to:
- Loosening of the implants
- Wear of the implants
- Infection
- Dislocation of the hip (the ball pops out of the socket)
- Fractures around the implants
- Allergic reactions
- Other issues
SHARED DECISION MAKING: TOTAL HIP REPLACEMENT
information coming soon ….